














































left sided stoma in crease

left sided stoma in crease
peristomal damage

peristomal damage
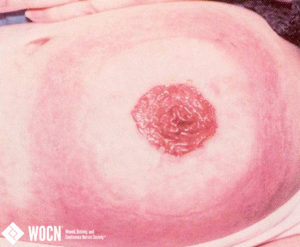
Broken down skin rash on African American patient

Broken down skin rash on African American patient
Psoriasis Colostomy

Colostomy with peristomal Psoriasis
Ileal Conduit Urostomy Acanthosis

Ileal Conduit/Urostomy with Acanthosis, urine ph >8
Loop Rod Problem 4

Loop Rod Problem 4 of 5
Loop Rod Problem 3

Loop Rod Problem 3 of 5
Loop Rod Problem 2

Loop Rod Problem 2 of 5
Loop Rod Problem 1

Loop Rod Problem 1 of 5
Loop Rod Problem, 5 of 5

Loop Rod Problem, 5 of 5
Uneven peristomal contours

Uneven peristomal contours
Stoma in skin fold 5 images
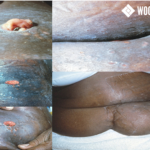
Stoma in skin fold 5 images
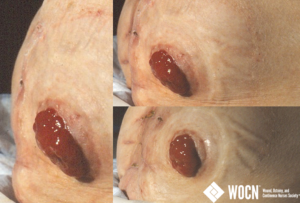
Uneven peristomal contours, 3 images
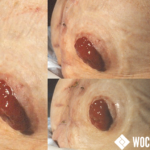
Uneven peristomal contours, 3 images
Ileostomy TapeMaceration NailTrauma

Ileostomy with tape induced maceration and digital trauma exacerbation.
HERNIA, FLUSH ILEOSTOMY STOMA - FRONT VIEW

Hernia, flush ileostomy stoma, low os, in lateral fold. 85 yo active female. Front view lying down. Shows that hernia looks less pronounced when lying down. Firm parastomal hernia more superior to ileostomy stoma area.
ILEOSTOMY HERNIA WITH APPLIANCE AND BELT

Ileostomy hernia with appliance and belt. Side view standing. 85 yo active female. Hernia makes pouching difficult for this patient. Belt helps hold pouch in place through position changes.
HERNIA, FLUSH STOMA - SITTING

Hernia, flush stoma, low os, in lateral fold. Front view sitting. 85 yo active female. Shows how much the parastomal hernia pushes stoma downward into the fold. Also makes it difficult for patient to pouch.
HERNIA, FLUSH STOMA

Hernia, flush stoma, low os, in lateral fold. 85 yo active female. Side view standing.
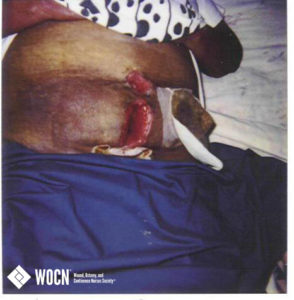
COLOSTOMY POST STOMA REVISION WITH OPEN ABDOMINAL WOUND

Colostomy secondary to ruptured diverticuli. Stoma revision and relocation performed with abdominal wound open from abscess. Has small EnterCutaneous fistula at inferior wound margin. Patient is African American, obese, Hypertensive and diabetic.
STOMA STENOSIS

Distal bowel has narrowed, necrosed and sloughed off creating this eventual obstipation of the bowel.
ILEOSTOMY WITH DEHISC ABDOMINAL INCISION

Ileostomy resulting from complication post hysterectomy. Dehisced abdominal incision secondary to seroma, treated with Negative Pressure Wound Therapy, Patient is African American, obese, diabetic, with a nonmalignant lypoma.
DENUDED PERISTOMAL SKIN

Peristomal skin is denuded, raw, weepy, dry flaky. (complication)
STOMA NECROSIS

Inadequate blood supply to stoma. Color is dark red, purple, brown or black with an odor.
CONTACT DERMATITIS

Open ulcers, erythema, pustules noted around area where appliance is placed. (complication)
HEALED PERISTOMAL ULCER

Scarring noted adjacent to an ostomy from a healed pressure ulcer that was caused by convex ostomy appliance and treated topically. (complication)
STOMA STENOSIS

Stenosis occurs when the distal bowel tissue is sloughed off. Stool has a ribbon appearance, which is the result of a narrowing opening.
PARASTOMAL HERNIA

Established Ileal Conduit (urostomy) with large peristomal hernia. (complication)
PERISTOMAL PRESSURE ULCER

Peristomal hernia and shallow, red ulcer possibly caused from pressure. (complication)
RETRACTED STOMA

Stoma is below skin level, may appear “hidden” in skin fold. Note denuded peristomal skin, pouching problems often occur.
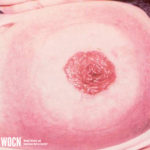
VIABLE BUDDED STOMA

Stoma is pink, budded, raised.
MECHANICAL INJURY

Partial thickness skin loss. Improper removal of appliance.
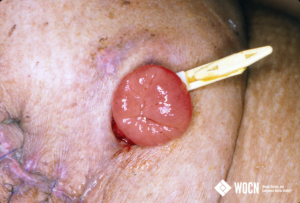
STOMA PROLAPSE

Bowel protrudes through the stoma, taking on an elongated shape. Stoma is red and healthy.
MUCOCUTANEOUS SEPARATION

Separation of sutures and skin at juncture, may appear as open areas with depth, sloughy or stool-stained. Stoma appears to be retracting into abdomen. (complication)
RETRACTED STOMA

Stoma is flush with skin.
STOMAL LACERATIONS

Shallow, linear, white/yellow ulceration.
PARASTOMAL HERNIA

Note: flush stretched stoma.
STOMAL PROLAPSE

Ostomy with prolapse and parastomal hernia. (complication)
PSEUDO-MEMBRANOUS COLITIS

Patient was admitted with a UTI and abdominal pain. The stoma was found with white patches that would de-roof when cleansed with a wash cloth. Blood was found in the pouch, intermittent diarrhea, abdominal pain and had been on several regimens of antibiotic treatments. WBCs were WNL, stool was tested for C-diff which came back negative. Patient was discharged on 14 days of Flagyl. Image taken: 9/2013
ALLERGIC DERMATITIS

Red, irritated area in shape of ostomy wafer.
NECROTIC STOMA

Blood supply to distal bowel is compromised which results in necrotic bowel. Serosa and subcutaneous tissue is compromised.
ULCERATED STOMA

Damage to stoma tissue, which can occur with poorly fitting appliance or trauma with appliance change.
IRRITANT DERMATITIS

Peristomal skin irritation.
PERISTOMAL ULCERATION

Ulcerated and broken skin around stoma which creates pouching problems. (complication)
RETRACTED, STENOSED STOMA

Stoma, which developed retraction and stenosis following necrosis and sloughing. Redness around stoma is cellulitis.
PERISTOMAL DERMATITIS

Skin redness from allergy or irritation (complication)
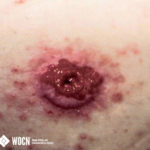
PERISTOMAL HYPERPLASIA

Raised lesions with warty appearance centered around the base of the stoma with a possible diffused circumferential pattern. (complication)
MECHANICAL INJURY

Peristomal skin is bruised, with ulcers, bleeding, and trauma resulting in epidermal shearing. (complication)
STOMA WITH DIFFICULT POUCHING SURFACE

Note skin folds and lack of level skin area for pouch to adhere to. (complication)
PERISTOMAL FOLLICULITIS
Hair follicles become infected and may present with pustules, erythema, lesions pain. (complication)
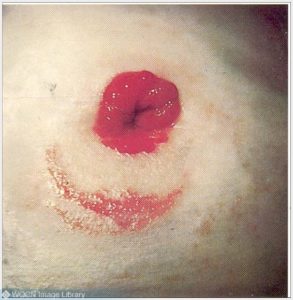
OSTOMY IN A CREASE WITH SECONDARY CONTACT DERMATITIS

Ostomy in a crease with leakage causing contact dermatitis. (complication)
ALLERGY TO POUCHING ADHESIVE
Distinct red circumferential pattern around stoma. (complication)
CAPUT MEDUSAE

Dilated vessels or varices caused by liver disease/portal hypertension at ostomy site. (complication)