The National Quality Forum (NQF) first published the Serious Reportable Events (SRE) List in 2002, updated it in 2011, and revised it again in 2026. For each iteration of the SRE list, NQF convened experts to identify a consensus-based subset of patient safety incidents that are not only largely preventable but also cause serious harm and should never occur in healthcare settings. Many states and healthcare organizations use the SRE List today for both mandatory and voluntary SRE reporting. SRE 21 has replaced SRE 15 in the 2025 Updates to Sentinel Events and Serious Reportable Events by the Joint Commission and National Quality Forum.
1. Definition of “Harm”
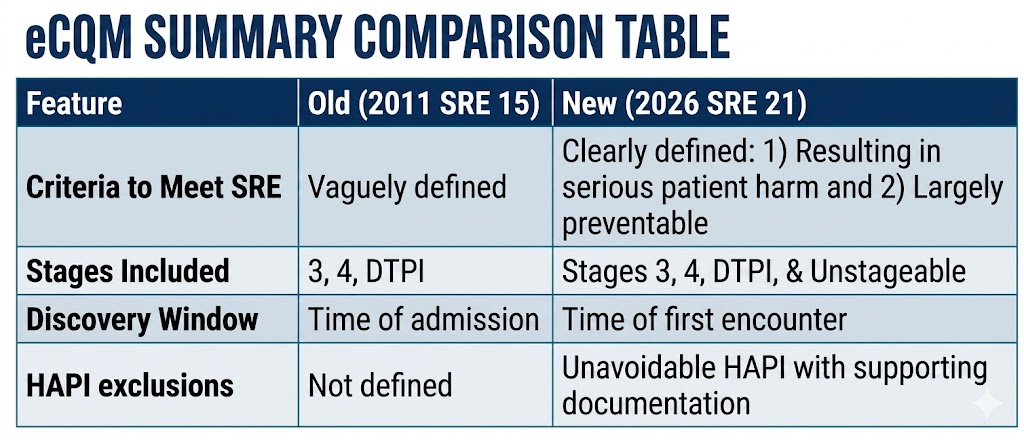
The clinician must establish if the pressure injury (PI) resulted in serious patient harm resulting in death or contributes to serious patient harm including physical, emotional, or psychological harm(s), that required major intervention (e.g., surgery, higher level of care, or treatment post-discharge) or impaired a patient’s ability to perform activities of daily living (ADL).
2. Definition of “Largely Preventable”
The clinician must establish if patient harm associated with a Stage 3 pressure injury, Stage 4 pressure injury, unstageable pressure injury, or deep tissue pressure injury acquired after admission was likely avoidable by any means currently available within the generally accepted performance standards of care or if the event triggers further analysis into causative factors.
Things to consider: Does documentation indicate all evidence-based pressure Injury prevention standards of care were met and performed? Setting-specific standards of care may include but are not limited to policies, procedures, or guidelines for skin assessment and documentation practices, implementation and documentation of defined prevention strategies, assessment and documentation of risk factors, and implementation of individualized care plans for complex medical conditions.
3. HAPI Stages Expanded
SRE 21 captures patient harm associated with the development of a new Stage 3 pressure injury, Stage 4 pressure injury, or unstageable pressure injury that develops after the initiation of a patient encounter and is not documented as present on admission
4. Specific “Clock” for Discovery (The 24/72 Rule)
SRE 21 adds strict timeframes to determine if a wound is truly “hospital-acquired”. Identification of hospital-acquired pressure injury (HAPI) begins at the time of the encounter, not just at admission, and it not limited to the time of admission to a unit or based on admission status (e.g., inpatient, observation). This also applies to extended emergency department boarding, emergency department to emergency department transfers, and observation stays.
To establish the occurrence of SRE 21, skin assessment documentation to create the baseline condition of the skin should occur at the start of the patient encounter.
- Hospital-Acquired Stage 3, 4, or Unstageable: Must be identified >24 hours after beginning of encounter to be an SRE.
- Hospital-Acquired Deep Tissue Pressure Injury (DTPI): Must be identified >72 hours after beginning of encounter.
5. Can we Exclude any PI?
SRE 21 acknowledges the “unavoidable” nature of some clinical conditions. It provides examples of situations where the HAPI MAY be excluded from reporting as an SRE, but documentation must support the exclusion. Examples include:
- Hemodynamic Instability: Patients on vasopressors or ECMO where turning is life-threatening.
- Unstable spinal fractures or open chests.
- Pre-admission Factors: Explicitly mentions “prolonged interfacility transport” (the “ambulance ride”) as a documented reason why a PI might be unavoidable.
- Refusal of preventative measures in instances such as end-of-life care.
- Skin changes at end-of-life